ĪĪ
J Gerontol A Biol Sci Med Sci. Author manuscript; available in PMC 2009 Feb 20.
Published in final edited form as:
J Gerontol A Biol Sci Med Sci. 2006 Jun; 61(6): 575©C584.
Interleukin-6 in Aging and Chronic Disease: A Magnificent Pathway
Marcello Maggio,1 Jack M. Guralnik,2 Dan L. Longo,1 and Luigi Ferrucci1
Author information Copyright and License information Disclaimer
1 Clinical Research Branch, Longitudinal Studies Section, National Institute on Aging, National Institutes of Health, Baltimore, Maryland
2 Laboratory of Epidemiology, Demography, and Biometry, National Institute on Aging, Bethesda, Maryland
Abstract
The human interleukin IL-6 was originally cloned in 1986. In 1993, William Ershler, in his article Ī░IL-6: A Cytokine for Gerontologists,Ī▒ indicated IL-6 as one of the main signaling pathways modulating the complex relationship between aging and chronic morbidity. Over the last 12 years, our understanding of the role of IL-6 in human physiology and pathology has substantially grown, although some of the questions originally posed by Ershler are still debated. In this review, we will focus on IL-6 structure, IL-6 signaling, and trans signaling pathways, and the role of IL-6 in geriatric syndromes and chronic disease. In the final section of this review, we dissect the critical elements of the IL-6 signaling pathway and point out targets for intervention that are targeted by emerging drugs, some still on the horizon and others already being tested in clinical trials.
Premises and a Brief History of Il-6
IN 1986, Kishimoto and collaborators cloned a DNA encoding a new human interleukin, BCDF/BSF-2, which was later named interleukin-6 (IL-6) (1). The extramembrane (IL-6r) and intramembrane (gp130) domain of the IL-6 receptor were characterized, respectively, in 1986 and 1988 (2,3). Since then, the interest in IL-6 in human physiology and pathology has increased exponentially. In 1993, William Ershler, in his article Ī░IL-6: A Cytokine for Gerontologists,Ī▒ indicated IL-6 as one of the main signaling pathways implicated in aging and chronic morbidity (4). ErshlerĪ»s intuition turned out to be prophetic.
Over the last 12 years, our understanding of the production and biological activity of IL-6 has substantially improved, and the role of IL-6 in aging and age-related conditions is now clearly established. However, some of ErshlerĪ»s questions are still in search of an answer.
Here, we review what is known about IL-6 structure, mechanism of action, and role in human pathology, focusing on what has been learned since the publication of the landmark Ershler article. Inflammation as a cardiovascular risk factor will not be addressed because this topic has been discussed in many other reviews (5). Specifically, we touch on trans signaling, the controversial debate on the proinflammatory versus antiinflammatory role of IL-6, and the role of IL-6 in several geriatric syndromes as well as in chronic inflammatory diseases. Finally, while discussing the critical elements of the IL-6 signaling pathway, we point out potential targets for intervention for emerging drugs, some already being tested in clinical trials and others still in the stages of development.
Structure and Signaling Pathways of Il-6: A Wonderful Complexity
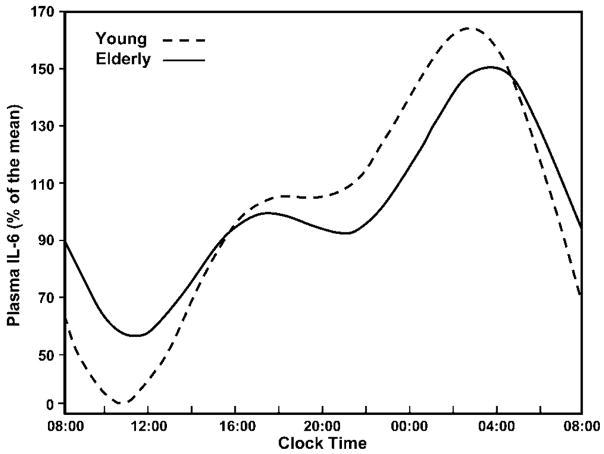
IL-6 is a helical glycoprotein with a molecular weight from 20 to 30 kD (1). Under physiologic conditions, the main source of IL-6 are cells of the immune system, vascular endothelial cells, and adipocytes. The concentration of IL-6 in the serum follows a circadian rhythm (6©C9) (Figure 1).
Figure 1
Interleukin (IL)-6 circadian rhythm. In both young and older persons, the secretion of IL-6 follows a circadian rhythm with two nadirs at about 8.00 and 21.00, and two zeniths at about 19.00 and 5.00.
IL-6 Production
IL-6 expression is mainly modulated by the nuclear factor kappa B (NF-KB). NF-KB proteins are maintained in the cytoplasm by their binding with inhibitory proteins (IKBs). A number of different stimuli, including cytokines, infections, and toxins, induce the phosphorylation, ubiquitinization, and subsequent degradation of the IKB protein by the proteasome. The degradation of IKB allows NF-KB to translocate to the nucleus and bind cognate DNA-binding sites to regulate the transcription of a large number of genes, including inflammatory cytokines (7,10©C13).
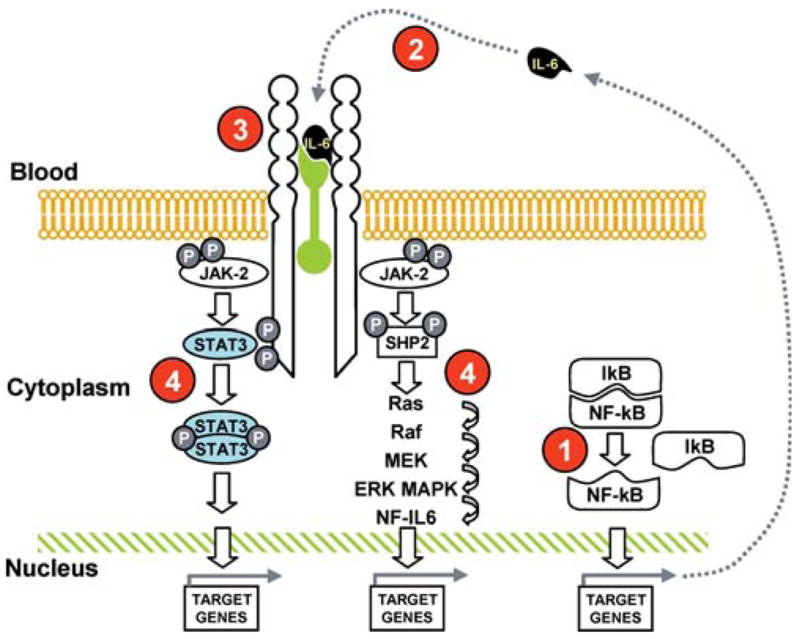
The IL-6 receptor consists of two glycoprotein subunits: an 80 Kd cognate receptor subunit (IL-6r, CD126), which specifically recognizes IL-6, and a 130-Kd signal-transducing element (gp130), which is the ubiquitously expressed signaling receptor molecule for the IL-6 family. The binding of IL-6 to IL-6r is followed by the homodimerization of gp130 and activation of two distinct signaling pathways: 1) the gp130-associated cytoplasmatic Janus and tyrosine kinases (JAK1, JAK2, and TYK2) signal transducers and activators of transcription (STATs, particularly STAT 1 and 3), and 2) the Src homology 2-containing tyrosine phosphatase (SHP-2)/extracellular signal-regulated kinase (ERK)/mitogen-activated protein kinase (MAPK) pathways (14©C16) (Figure 2).
Figure 2
Interleukin (IL)-6-signaling pathways with potential drug targets. Two different pathways: phosphorylation of Janus kinase 2 (JAK2), phosphorylation and dimerization of signal transducer and activator of transcription 3 (STAT3) with successive translocation of STAT3 to the nucleus, and transactivation of target genes (STATs remain in the cytoplasm until they are activated by JAK); activation of the Ras-Raf pathway, which regulates phosphorylation of mitogen-activated protein kinase (MAPK), whose substrate is nuclear factor IL-6 (NF-IL-6). Note that two different IL-6-responsive elements exist in the promoter region of the acute-phase protein genes targeted by NF-IL-6 and STAT3 (13©C15). The numbers in red indicate the potential drug targets and are discussed in the text.
IL-6 Trans Signaling and Actions
While the cognate IL-6r (CD126) is only expressed by hepatocytes, neutrophils, monocytes/macrophages, and specific lymphocyte subpopulations (17), IL-6 affects many more cell types. This is possible because IL-6r exists in a soluble form (sIL-6r), which can bind IL-6 and form a circulating IL-6/sIL-6r complex that can cause the dimerization of the ubiquitous gp130, even in cells that do not have IL-6r. Soluble IL-6r is formed by proteolytic shedding from the surface of neutrophils and monocytes or splicing during the transcription of the IL-6r gene (18,19).
The shedding process is stimulated by several factors including C-reactive protein (20) (which through this mechanism amplifies the IL-6 signaling), IL-8 (21), and cellular cholesterol depletion (22), and blocked by a metalloprotease inhibitor and tumor necrosis factor (TNF)-alpha protease inhibitor (TAPI) (23).
Factors that stimulate the production of the spliced form are still not well understood. The activation of the IL-6 pathway by the IL-6/sIL-6r, known as Ī░trans signaling,Ī▒ accounts for most of IL-6 biological activity and is a unique example of a cytokine-soluble receptor with agonistic instead of antagonistic properties (24,25).
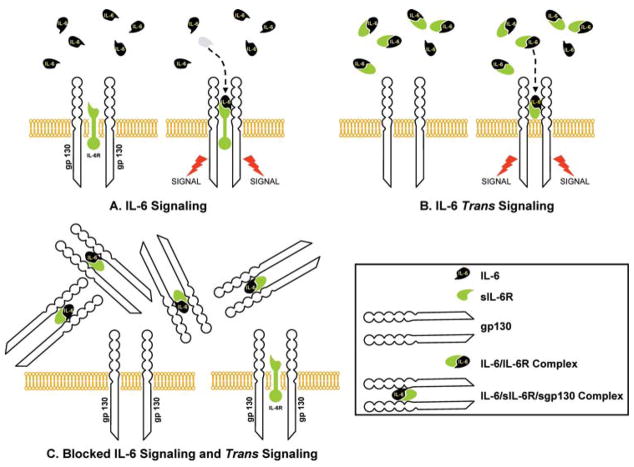
The trans signaling mechanism is regulated by a soluble form of gp130 (sgp130), which can bind and completely inactivate the IL-6/sIL-6r complex (26,27) (Figure 3). IL-6/sIL-6r complex can also up-regulate the gp130 expression in certain cells, such as smooth muscle cells (28).
Figure 3
Interleukin (IL)-6 signaling and trans signaling. The IL-6 receptor consists of two glycoprotein subunits: a cognate receptor subunit (IL-6r) and a 130-kD signal-transducing element (gp130). IL-6 binds the IL-6 receptor and activates the signal (A). The IL-6r can be shed from the membrane of the IL-6-sensitive cell and becomes soluble IL-6r. Soluble IL-6r (sIL-6r) binds IL-6 and forms IL-6/sIL-6r complex, which is able to activate the IL-6 signal. This process is known as Ī░trans signalingĪ▒ (B). A soluble form of gp130 binds and completely inactivates the IL-6 complex. As a consequence, cells with transmembrane gp130 remain insensitive to IL-6 (C).
IL-6 serum concentration, which is usually in the low pg/ml range, may increase 1000 fold, beyond 5 ng/ml (29). Conversely, levels of sIL-6R and sgp130 fluctuate much less (30). When IL-6 concentration rises, the percentage of IL-6/sIL-6r bound to gp130 progressively declines and the biological activity of IL-6 increases (27,30,31). Although the relevance of the modulator mechanism mentioned above in human physiology and pathology is still under investigation, it is already clear that a base measure of IL-6 provides little information on the degree of activation of the IL-6 pathway.
In animal models of chronic inflammatory disease of the gastrointestinal tract, the blockade of the IL-6 trans signaling caused T-cell apoptosis, indicating that the IL-6/sIL-6r contributes to the perpetuation of chronic intestinal inflammation (32). Accordingly, in a randomized controlled trial, the administration of a human anti-sIL-6r monoclonal antibody in patients with CrohnĪ»s disease reduced the circulating levels of acute-phase reactants and resulted in slight clinical benefit (33). These findings are probably not disease specific and are consistent with the current view that the early phases of inflammation (neutrophil response, acute phase reactants) is mediated by CD126 signaling, and the transition to cell-mediated immunity is mediated by IL-6 trans signaling, perhaps through the prevention of T-cell apoptosis (32).
Il-6 As an Inflammatory Mediator
The physiological role of IL-6 has been mostly studied in the context of the acute phase response, although there is growing evidence that IL-6 also plays a central role in the pathogenesis of chronic disease (17). In acute inflammation, IL-6 promotes the expansion and activation of T cells and differentiation of B cells, and modulates the synthesis of positive (such as C-reactive protein and fibrinogen) and negative (such as albumin) acute phase reactants (34©C37). Other typical manifestations of acute inflammation, such as fever, activation of the hypothalamic©Cpituitary©Cadrenal axis, anorexia, and lethargy are similarly induced by IL-6 (34). Interestingly, recent studies also suggest that one of the main functions of IL-6 is self-limiting the inflammatory response by suppressing the production of TNF-alpha and IL-1 beta (38,39) and increasing the synthesis of IL-1 receptor antagonist (IL-1 Ra) and soluble TNF receptor p55 (40). In addition, IL-6 confines neutrophil recruitment, favoring their replacement by mononuclear cells (41). In animal models, this effect is present during septic shock (42). Thus, IL-6 concomitantly regulates proinflammatory and antiinflammatory activities and contributes to both the development and the resolution of the acute inflammatory response. The switch from the inflammatory burst that follows an inflammatory stimulus to the chronic elevation of IL-6 typical of immune-mediated diseases and encountered in many older persons is much less understood. As mentioned above, there is evidence that, at least in some specific pathological conditions, the transition to a chronic inflammatory state is sustained by IL-6 trans signaling. However, a fundamental question remains of whether elevated levels of IL-6 are aimed at resolving an inflammatory response that is inappropriately long or whether a primary dysregulation of IL-6 production is responsible for a chronic proinflammatory state, which has a negative impact on health status. Future studies that evaluate the effects of blocking the IL-6 signaling in older persons affected by a chronic proinflammatory state and different patterns of comorbidity may shed light on this question.
Age-Related Changes in Il-6 and Il-6 Receptors
There is strong evidence that IL-6 serum concentration increases with age (43©C50). We reported that IL-6 mean values ranged from 1.4 pg/ml (men) and 1.1 pg/ml (women) in the 65©C74 years age group to 3.5 pg/ml (men) and 2.1 pg/ml (women) in persons 85 years and older, and that the age trend is partially independent of major confounders (50). Age-related increments in IL-6 are not explained by differential prevalence of IL-6 gene polymorphisms (51), while there is evidence that the excessive production or reduced clearance of oxygen free radicals, which stimulate IL-6 production, may be important (52). Giuliani and colleagues observed a significant increase of sIL-6r up to the seventh decade followed by a gradual decline (53). However, because of inconsistent findings, understanding the effect of age on circulating levels of sgp130 and sIL-6r requires further investigation.
Il-6, Adipose Tissue, Muscle, and Insulin Resistance
IL-6 is produced in skeletal muscle. Physical exercise produces a 10-fold increase in serum IL-6, mostly released from skeletal muscle and perhaps aimed at potentiating the insulin stimulation of glycogen synthesis in muscle cells (54,55). Body composition is also another important correlate of IL-6, especially the percentage of visceral fat. IL-6 produced by omental adipose tissue accounts for 10% to 35% of the bodyĪ»s basal circulating IL-6 level (56,57). Because of the relationship with adiposity, it has been hypothesized that IL-6 and other proinflammatory cytokines are the main cause of insulin resistance. Interestingly, while the epidemiological evidence supporting this hypothesis is compelling, experimental studies failed to demonstrate the existence of such a mechanism (58).
It has even been suggested that IL-6 attenuates the insulin signal in energy supply tissues (liver, fat), whereas it enhances insulin action in energy-utilizing tissues (skeletal muscle) (54). In vivo and in vitro studies provide evidence for this hypothesis, suggesting that IL-6 signaling can induce a rapid and transient phosphorylation of insulin receptor substrate (IRS-1) in cultured skeletal muscle cells and in muscle tissue, but not in the liver. Of note, two inhibitory mechanisms of IL-6 on insulin action (phosphorylation of the inhibitory Ser-307 residue of IRS-1 and induction of SOCS-3 [suppressor of cytokine signaling 3] expression) have been found in liver, but not in muscle of IL-6-treated mice (59).
Effects of Diet and Exercise on Il-6 Secretion
Diet may affect IL-6 secretion both acutely and chronically. A high-fat meal, but not a high-carbohydrate meal, increases plasma levels of IL-6, and the magnitude of the increment is attenuated by a premeal ingestion of vitamin E and ascorbic acid (60). Circulating levels of polyunsaturated fatty acids, especially total n-3 fatty acids, are independently associated with lower levels of proinflammatory markers, including IL-6. Moreover, consuming a Mediterranean diet is associated with significantly lower IL-6 (61,62).
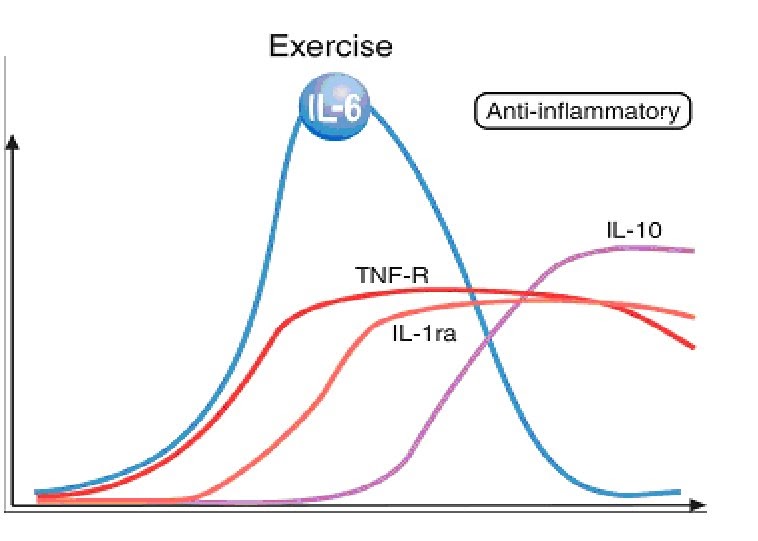
Plasma IL-6, but not TNF-alpha, increases during acute exercise in proportion to intensity, duration, and level of fitness. It has been suggested that IL-6 is important for the process of muscle repair and cell turnover, as well as for some of the beneficial health effects of exercise, especially on lipids (63). In contrast to these acute effects, persons who are chronically physically active tend to have lower levels of IL-6 and other inflammatory markers (64). A combined intervention of low-calorie diet and exercise significantly reduced circulating and tissue (adipose tissue) IL-6 levels (65).
ĪĪ
Il-6 and Osteoporosis
IL-6 has potent antiapoptotic properties on osteoblasts (66) and may affect osteoclast development (67), both of which could lead to osteoporosis. In addition, IL-6 induces bone resorption by multiple mechanisms (68,69). In animal models, estrogens inhibit IL-6 gene expression, and blocking estrogens increases IL-6 and bone resorption (70). Interestingly, transgenic mice over-expressing IL-6 do not have osteoporosis (71). However, human studies show that IL-6 and sIL-6r levels are negatively associated with bone mineral density, and the IL-6 gene is an independent predictor of bone mineral density and peak bone mass (53,72,73).
Il-6 and Sex Hormones
Recent studies suggest that declines in the production and circulating levels of steroid hormones contribute to the mild proinflammatory state typical of older persons. For example, dehydroepiandrosterone (DHEA) and DHEA sulphate are negatively correlated with serum IL-6 and inhibit IL-6 secretion from human mononuclear cells (74). An effect of estrogens on IL-6 is also suggested by the detection of increased levels of IL-6, sIL-6r, and sgp130 after natural and surgical menopause (7,75©C78) and increased postovariectomy sIL-6r levels (35%), which can be prevented by estrogen replacement (76). Additionally, low-dose estrogen treatment in postmenopausal women causes a reduction in IL-6 and sIL-6r circulating levels (76,79,80), which, in some cases, is paralleled by improvement of hip and lumbar spine bone mineral density (81).
Although studies examining the effect of testosterone on IL-6 have produced conflicting results, the addition of testosterone to cell cultures down-regulates IL-6 production in human macrophages (82) and in murine (83) and human cultured osteoblasts (84). In male participants of the InCHIANTI study population living in Tuscany (Italy), we found a significant, inverse independent association of bioavailable and total testosterone with sIL-6r, but not IL-6 and other inflammatory markers (85). Similarly, Khosla and coauthors found that antiandrogen treatment in men increased IL-6 and sIL-6r levels, and testosterone partially reverses this effect (86). The administration of testosterone partially prevents the rise in IL-6 that occurs after a coronary stenting (87). Surprisingly, two recent studies did not find any significant reduction in IL-6 serum levels after testosterone administration in older and postpubertal hypogonadal men (88,89).
The mechanism whereby DHEA, estrogens, or testosterone inhibit IL-6 gene expression is not understood. In fact, there are no estrogen or androgen response elements in the putative promoter region of the IL-6 gene. A clue for the underlying mechanism comes from recent data suggesting that androgens inhibit the transmigration of NF-KB from cytoplasm to nucleus (90,91).
Il-6: Fuel for Frailty and Disability
The possible causal role of IL-6 in frailty, sarcopenia, and disability is a fascinating but still unsolved research question (92). Frail study participants have higher levels of IL-6 than nonfrail, age-matched individuals (93). Elevated serum IL-6 is positively associated with markers of physical frailty such as low walking speed, poor muscle strength (94), poor lower extremity performance (95), and anemia (96), even after adjustment for confounders.
IL-6 levels are cross-sectionally associated with disability in community-dwelling elderly persons (48) and are predictive of future disability in nondisabled older persons (97). We showed that most of the relationship between IL-6 and disability is accounted for by the detrimental effect of IL-6 on muscle strength (97). IL-6 may contribute to sarcopenia through different mechanisms, including a direct interference with insulin signal transduction and inhibition of the production and biological activity of insulin-like growth factor-1 (IGF-1) (98,99). Interestingly, low IGF-1 and IL-6 levels were independent and almost synergistic risk factors for disability both in the WomenĪ»s Health and Aging Study I and in the InCHIANTI Study (99,100).
In animal studies, IL-6 infusion results in muscle atrophy characterized by a preferential loss of myofibrillar protein (−17%), perhaps secondary to SOCS activation and to increased STAT phosphorylation in favor of a more catabolic profile (101).
Finally, it has been suggested that the core mechanism leading to age-associated frailty is excessive and unopposed oxidative stress, and, therefore, high IL-6 in frail older persons is only a marker of this phenomenon with little causal pathophysiologic role. The direct testing of this hypothesis is difficult because biomarkers of oxidative stress have limited reliability and validity (102).
ĪĪ
Il-6 in Chronic Disease
IL-6 and Cancer
IL-6 is a growth/survival factor for a variety of tumor types. Activation of STAT3 by IL-6 is correlated with increased antiapoptotic (the bcl family), cell cycle gene expression and activation of androgen receptor genes. An extensive literature search suggests that IL-6 has a role in multiple myeloma and prostate and ovarian cancers. In addition, there is evidence that the excessive production of proinflammatory cytokines, including IL-6, accounts for tumor-related constitutional symptoms and associated cachexia (103©C107).
Uncommon Conditions Where IL-6 Plays a Special Role
Three specific medical conditions (cardiac myxoma, CastlemanĪ»s disease, and multiple myeloma) warrant special examination in the context of IL-6 and disease pathogenesis. Cardiac myxoma, a benign atrial heart tumor, produces large quantities of IL-6, which cause autoantibody production, fever, joint pain, and anemia (108). Described by Dr. Benjamin Castleman in 1956, CastelmanĪ»disease is a relatively rare lymphoproliferative disorder caused by human herpes virus 8, whose genome encodes a viral IL-6, which causes most of the associated symptoms (109). Elevated levels of IL-6 in multiple myeloma protect tumor cells from glucocorticoid-induced death (105) by activating STAT 3-dependent antiapoptotic genes (110). Confirming the importance of trans signaling, sIL-6r is significantly elevated in myeloma patients and correlated with the disease severity (36,37,111©C114).
IL-6 and Diabetes
The role of IL-6 on beta cell survival and type 1 diabetes is probably small (115©C119). On the contrary, observational studies show that IL-6 is a risk factor for type 2 diabetes (120©C122). Whether increased IL-6 is causal or merely reflects an attempt by the body to counteract low-grade inflammation, mirrored by elevation of other inflammatory markers, resulting from diabetes is still an open question.
IL-6 and Hypoproliferative Anemia
IL-6 in concert with other proinflammatory cytokines is the primary cause of anemia of inflammation, formerly defined as the anemia of chronic disease (123). Recent preclinical studies suggest that IL-6 stimulates hepatocytes to produce hepcidin, a polypeptide that inhibits intestinal absorption and reticuloendothelial release of iron (124). However, there is evidence that IL-6 may cause anemia through other mechanisms, including rapid hemodilution, down-regulation of the membrane-bound erythropoietin receptor, and impairment of erythroid proliferation and maturation (125©C127).
IL-6 and CrohnĪ»s Disease
In CrohnĪ»s disease (CD), serum and intestinal levels of IL-6 and sIL-6r are higher than in controls (128,129) and correlate with the severity of inflammation (128,130). Accordingly, the IL-6-dependent STAT3 is highly phosphorylated (131), and lymphocyte gene expression of IL-6r and gp130 are enhanced (132).
Interestingly, IL-6 trans signaling protects mucosal T cells against apoptosis contributing to the perpetuation of chronic intestinal inflammation. Blockade of IL-6 trans signaling causes T-cell apoptosis and symptom improvement (32).
IL-6 and Rheumatoid Arthritis
SKG mice that spontaneously develop rheumatoid arthritis (RA) are completely protected from the disease if the IL-6 gene is knocked out, suggesting that IL-6 is critical to the pathophysiology of RA (133). Accordingly, sIL-6r and IL-6 levels are increased in the synovial fluid and the serum of RA patients and are highly correlated with disease activity (134©C136).
IL-6 and AlzheimerĪ»s Disease
In vitro, endogenously produced cytokines could influence beta amyloid peptide accumulation and tangle formation. Conversely, beta amyloid and tau proteins stimulate microglia, astrocytes, and oligodendrocytes to overproduce inflammatory mediators, therefore generating a Ī░vicious cycleĪ▒ leading to irreversible synaptic loss (137). In spite of this rationale, observational studies looking at specific patterns of elevated cytokines, such as IL-6, sIL-6r, and sgp130, in serum and in cerebrospinal fluid of AD patients have produced conflicting results (138,139).
From Bench to Bedside
Therapeutic Strategy Targeting IL-6-Signaling Pathways
In Figure 2, we outlined the elements of the IL-6 production and signaling pathways. Pharmacological intervention can modulate the IL-6 signaling pathways by interfering with different critical steps.
1. Proteasome and NF-KB
The proteasome, a multi-catalytic proteinase complex, is responsible for the majority of intracellular protein degradation. Proteasome inhibitors block the degradation of IKB, thereby sequestering NF-KB in the cytoplasm and preventing its protranscriptional activity (140,141). Bortezomib, the first proteasome inhibitor to undergo clinical testing, has significant efficacy against multiple myeloma and non-HodgkinĪ»s lymphoma (142).
Thalidomide and thalidomide analogues also down-regulate NF-KB activity, together with inhibiting the P13K/AKT and JAK/STAT (143). This therapeutic approach is currently been tested in a pilot project at the National Institute on Aging targeting frail participants.
2. Targeting IL-6
IL-6-neutralizing monoclonal antibodies (BE-8 and CNTO) are currently being tested in six early stage clinical trials performed in B-cell lymphoproliferative disorders, primary central nervous system lymphoma (primary cerebral lymphoma), multiple myeloma, and renal cell carcinoma. In preliminary studies, these compounds have shown dramatic reduction of C-reactive protein and improvements of cancer-related symptoms (fever, cachexia, and pain) (103). A novel series of IL-6 antagonists called Sants (super antagonists) antagonize receptor binding without activating the IL-6 signaling cascade (144) and induce cell cycle arrest in primary myeloma cells (145,146). These molecules are still in an early development stage and have not been tested in human studies.
3. Targeting IL-6 receptor
Tocilizumab, a humanized anti-IL-6 receptor antibody, is the most-studied intervention targeting sIL-6r in chronic inflammatory diseases (147,148). Pilot and full-scale randomized clinical trials are currently being conducted for the treatment of CrohnĪ»s disease (33), rheumatoid arthritis (149), moderately active systemic lupus erythematosus (150), and CastelmanĪ»s disease (151,152).
Overall, tocilizumab administered for 4 to 60 weeks, at a daily dose of 2©C8 mg/kg, was well tolerated and significantly improved inflammatory parameters in all diseases in which it was employed. The major side effects were an increase in lipid levels, which returned to normal values after treatment was withdrawn. The long-term safety of tocilizumab is still under investigation.
Recent observational and preliminary intervention studies suggest that the administration of soluble glycoprotein 130 may significantly reduce the severity of arthritis (153,154), probably by inactivating the IL-6/sIL-6r circulating complex.
4. Targeting JAK-STAT and JAK-MAPK
AG-490 (Tyrphostin) and Cucurbitacin I (JSI-124) are active against the JAK, the latter showing moderate selectivity for JAK2 (155,156). These molecules have not been tested in clinical trials. Studies on the pathway leading to apoptosis in myeloma cells showed that the Farnesyl transferase inhibitors R11 5777 inhibit MAPK, PI3K-AKT, and JAK/STAT pathways through inhibition of STAT3 and ERK1/2 (157,158).
Statins, curcumin, and cucurbitacin Q have been shown to decrease IL-6-induced CRP expression in human hepatocytes at the transcriptional level by reducing phosphorylation of STAT3 (159©C161). No studies, with the exception of statins, in humans are available.
Lys685 acetylation is critical for STAT3 to form stable dimers required for cytokine-stimulated DNA binding and transcriptional regulation, to enhance transcription of cell growth-related genes, and to promote cell cycle progression. The identification of compounds that affect Lys685 acetylation is currently under development. There is in vitro evidence that Paclitaxel, a microtubule stabilizer, selectively inhibits STAT3 translocation (162). New short peptides called aptamers interact with STAT3 dimerization domain and inhibit DNA binding and transactivation (163). However, aptamers specific for IL-6 are not currently available. Gene transcription is another potential target of IL-6 modulation, and compounds such as transcription factor decoy, SiRNA, and antisense are under investigation.
Opening Questions for a Research Agenda
Since ErshlerĪ»s landmark article, our understanding of the IL-6-signaling pathway and its role in the development of a late-life, mild proinflammatory state, chronic morbidity, and frailty has grown tremendously. However, studying IL-6 has been similar to opening a PandoraĪ»s box, we have generated many more new questions than definitive answers.
From a gerontological perspective, we believe that the most burning of the many possible questions are the following:
To clarify how the complex interaction between the relative concentrations of IL-6, sIL-6r, and gp130 affect the degree of activation of the IL-6 pathway in different cell types.
To understand the mechanisms that cause the switch from an acute inflammatory response to a chronic inflammatory state, particularly in reference to the mild proinflammatory state of aging.
To sort out the proinflammatory and antiinflammatory properties of IL-6 and how they are affected by patterns of concentration of biomarkers involved in the regulation of biological homeostasis.
To understand the relationship between health-related behaviors, in particular nutrition and physical activity, and the production of IL-6, sIL-6r, gp-130, and other inflammatory markers.
To test the hypothesis that a dysregulation in the IL-6 production and biological activity is central to the pathogenesis of frailty and, ultimately, whether treatment aimed at modulating the IL-6 pathway may prevent frailty or have positive effects in older frail patients.
To verify whether the mild proinflammatory state that often affects older persons is due to a primary dysregulation of the immune system or rather a reactive response to excessive and not adequately opposed oxidative stress.
Conclusion
The IL-6 pathway appears to be profoundly implicated in the pathophysiology of physical function decline and chronic diseases that often affect older persons. Because of this activity across multiple physiological systems, it is conceivable that a primary IL-6 dysregulation is the first step in the development of frailty. If IL-6 dysregulation is demonstrated to be a direct cause of physiologic decline with aging, rather than an innocent bystander reflecting some other process, then modulation of IL-6 production or effects could offer a major breakthrough in prevention and treatment of people at advanced old age.Interleukin-6 in Aging and Chronic Disease: A Magnificent Pathway
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2645627/ĪĪ